

THE FOOTMOTION PODIATRY TEAM
Dr. Lloyd Reed has over 30 years of ongoing clinical experience in podiatry, as well as holding senior academic and research positions. He has a wealth of expertise in both research and clinical care for the prevention and treatment of musculoskeletal disorders, foot problems in diabetes and in the workplace. Dr. Reed stepped down from heading up the podiatry department at QUT to lead the team at FootMotion Podiatry in 2015.
ASSOCIATE PROFESSOR DR. LLOYD REED Podiatrist
Podiatrist

Kerrie Dahler, is a compassionate podiatrist with over three decades of experience, specialises in foot pain treatment. At Footmotion Podiatry since 2021, she excels in biomechanical assessments and gait analysis, diagnosing conditions like plantar fasciitis, and offering evidence-based treatments such as orthotics and laser therapy. Kerrie prioritises patient-centered care, listening attentively and crafting personalised treatment plans collaboratively.
KERRIE DAHLER Podiatrist
Podiatrist

Nerylie has owned and worked in private practice for over 25 years. She has held a number of leadership positions on government, podiatry association, and Queensland Health committees and boards. Her clinical skills, particularly with the diabetic foot, are widely recognised and well sought after by her clients and acknowledged through her appointments over the past 14 years as a university podiatry clinical supervisor.
NERYLIE WHITECROSS Podiatrist
Podiatrist

After more than 20 years of nursing practice, Marylou completed a Bachelor of Applied Science (Nursing) in 1988, then to a Bachelor of Applied Science (Podiatry) in 1995. For 28 years as principal of her practice Toowong Podiatry, she provided the full range of General Care, especially to those patients with feet deemed "at risk" and suffering chronic disease. She feels privileged to continue to care for her patients as a part of the FootMotion Podiatry team.
MARYLOU THEARLE Podiatrist
Podiatrist

Hamish graduated from QUT with a Bachelor of Podiatry (Honours) and has since worked in both private practice and teaching roles at QUT. In late 2020 Hamish began his PhD, investigating plantar heel pain in athletes - a continuation of a lifelong interest in running and, more recently, cycling, biomechanics and injury. Hamish enjoys treating a mix of podiatry conditions alongside his particular interest in sports medicine.
HAMISH HARVEY Podiatrist
Podiatrist

Karina, who graduated from QUT in 2023 with First Class Honours in Podiatry, recently joined Footmotion's podiatry team in 2022. Her educational background in exercise science, coupled with her experience playing Division I college basketball in the United States, fuels her passion for biomechanics, sports rehabilitation, and gait analysis. Excited to contribute full-time, Karina aims to help people of all ages move freely and painlessly at Footmotion.
KARINA PELL Podiatrist
Podiatrist

Nina started working at FootMotion in 2023 as a podiatry assistant, before graduating QUT Bachelor of Podiatry with a distinction. She is interested in all aspects of podiatry, but has a particular passion for biomechanics and creating orthotics prescriptions.With her Mandarin skills, she looks forward to treating a wider population of patients.
NINA PENG Podiatrist
Podiatrist


Who We Are
FootMotion Podiatry is a team of caring and highly skilled podiatrists, dedicated to helping you solve your foot and lower limb problems.
At FootMotion, we are the foot pain specialists. We use our professional expertise and state-of-the-art software and equipment to help provide you with the highest level of care to match your needs.

Conditions We Treat
- Bursitis
- Foot Callus and Corns
- Bunions
- Plantar Fasciitis
- Arthritis & Gout
- Plantar Warts
- Heel Pain
- Fractured Toes & Ingrown Toenail
Our Services
- General Podiatry
- Gait Analysis
- Diabetes Foot Protection
- 3D Cadcam Orthoses
- Footwear Assessment
- Exercise Prescription
- Chronic Disease Management
- Balance Assessment

TALK TO OUR FRIENDLY TEAM
Call us today: (07) 3371 3300

Conditions
 WHAT IS BURSITIS?
WHAT IS BURSITIS?
Bursitis occurs when a bursal sac is inflamed. Bursal sacs are located throughout the body.
They are fluid filled sacs that help to lubricate and reduce friction between two surfaces in the body, usually muscles and tendons as they glide over bony prominences.
In the foot there is only one naturally occurring bursal sac, which is located between the Achilles tendon and the heel bone (calcaneus).
However in response to the constant “micro-trauma” that our feet experience when we walk, the body creates bursal sacs to protect areas of the foot where trauma is occurring. If the trauma continues, the bursal sac (that has formed in order to protect the foot) becomes inflamed and bursitis develops.
Symptoms include:
- Pain, inflammation, redness and swelling
- Heat may emanate from the painful area
- Increased pain in the morning, or after being immobile for extended periods of time
CAUSES
Bursitis in the foot is usually secondary to other foot conditions. For example:Bunion or tailor’s bunion
People who have a bunion or tailor’s bunion will often have bursitis on the side of the foot where the bony prominence is located.
Hammertoe
In the presence of a hammertoe, the condition may form on the top of the toe as it rubs on shoes. Symptoms of this include tenderness, redness and swelling on the top of the affected toe. With too much pressure the bursitis can burst and become infected.
Ball of foot pain
HOW IS IT TREATED?
Because it is often secondary to other foot conditions, it is important that treatment addresses any underlying foot condition (such as bunion deformity, hammertoe).
Additional treatment to relieve the symptoms of bursitis includes:
- Anti-inflammatory medication
- Icing the area
- Orthotics to redistribute body weight through the foot and take pressure off the painful area
- Footwear advice
 WHAT ARE CORNS AND CALLUSES?
WHAT ARE CORNS AND CALLUSES?
A corn is a more focal area of thick skin which has caused a cone shaped plug of skin that presses down on to sensitive soft tissue underneath the skin. The thicker and bigger they get, the more painful they can become. Corns can also occur anywhere on the foot but are particularly common around bony prominences such as toe joints and the joints in the forefoot. They may be round, slightly raised and may too feel rough, but look slightly darker than the callus. They can also occur between the toes, where they may take on a more rubbery appearance due to excessive moisture between the toes.
According to one of the largest research studies in this area, nearly one in 5 employees in a workplace setting had corns or callouses under the forefoot [1]. Assessment of 1000 podiatry patients attending a university clinic found that forefoot corns and callouses were more common in women, were more often painful as people became older and were most common under the heads of the first metatarsal (21%), the second metatarsal (29.8%) and third metatarsal (12%). [1] In an Australian study of older adults, 60% had at least one callous or corn beneath their feet.[2]
It is important to determine if your skin problem is a corn or callus or if it could be a plantar wart, as the treatments will be different in each case.
WHAT CAUSES CORNS AND CALLUSES?
Corns and calluses form usually in response to too much pressure, arising from prominent joints or from too much rubbing or friction. This can be caused by:
- Poor fitting or non-cushioned footwear
- Foot deformities such as bunions, hammer toe and claw toes
- Pronated feet that move too much within shoes
- High-arched feet with high forces at the forefoot and heel
- Older feet where the skin is less elastic and there is less fat pad to provide cushioning excessive weight
Corns and calluses can also be due to conditions such as psoriasis and rheumatoid arthritis. Care must be taken if you develop corns and callus and also have diabetes as they can lead to development of serious complications such as foot ulcers. People with diabetes should have regular foot assessments by podiatrists.
At FootMotion, we use our extensive clinical experience and state-of the-art technology to properly diagnose your skin condition, carry out a thorough vascular and neurological examination to accurately assess your foot health and create an evidence-based treatment plan to effectively manage your condition.
 HOW CAN CORNS AND CALLUSES BE TREATED?
HOW CAN CORNS AND CALLUSES BE TREATED?
Treatment for corns and callus should be aimed at both relieving your symptoms by removing the thick skin as well as reducing the excessive pressure or friction causing them in the first place.
Removing your corns and callus involves careful debridement using a sterile scalpel to gently remove the thick skin. This process is normally quite painless as the tissue being removed has no sensation. The area would then be smoothed using a file or sanding instrument. In some cases, your podiatrist may use chemicals called caustics or keratolytics to help remove the thickened skin. You will also be given advice on self-care using appropriate creams, padding and filing, to help prevent or manage the thickening of the skin.
While ever there is still too much pressure or friction, the corns and calluses will likely continue. That’s why your treatment plan at Footmotion may include:
- Prescription of supportive, well-cushioned footwear that is fitting well
- Shoe padding to offload specific areas of high pressure
- Arch supports or prescription orthoses to improve function and reduce pressure and friction
In many cases these measures may stop the corns and calluses completely but sometimes the problems are severe enough that the goal is to slow down the process, reduce/remove the pain and lengthen the time between treatments.
 WHAT ARE BUNIONS?
WHAT ARE BUNIONS?
Bunions - seen on the big toe Bunions are boney bumps that develop on the side of your foot just behind your big toe. The bump is caused by the alignment of the bones changing, with the big toe leaning over closer to the second toe, which forces the joint to shift outwards, making it more prominent. The medical term for bunions is hallux valgus (or HV). A similar bump can also develop on the other side of your foot behind the little toe – this is called a bunionette.
Bunions occur in around 23% of adults aged between 18 and 651, with women over two times more likely to develop them than men. This increases to as many as 35% in people older than 65 years. Children and teenagers are also susceptible to bunions (8%). It is vital to identify and manage bunions early, as the condition is progressive and the bunions will generally get worse with time.
Pain from bunions can be due to skin and soft tissue irritation and inflammation, both at site of the bunion as well as in other toes. As the bunion progresses though, pain can be more severe and cause symptoms in multiple foot joints as they become more damaged.
Aside from problems associated with finding comfortable shoes, other areas of your feet and legs can be affected, as well as your balance and the way you walk. Studies have also demonstrated that bunions can increase falls risks in older people. WHAT CAUSES BUNIONS?
WHAT CAUSES BUNIONS?
The realignment of bones in the foot cause bunions Bunions form due to an abnormal pull of the muscles around an unstable joint. Research suggests that the shape and position of certain bones in your feet may leave you more susceptible to bunions. In particular, the shape of the 1st metatarsal and the length of the first metatarsal bone seem to be associated with developing this condition.
It is also thought that the condition may be hereditary. It has previously been thought that poor footwear (including high heels) and flat feet may be causes. Conditions such as Rheumatoid Arthritis and other connective tissue disorders also appear to increase your risk of developing bunions. Conditions such as gout and hallux limitus can also cause pain and swelling of the big toe joint. In our clinic we see that the way people walk can also be a factor. When the foot rolls in or ‘pronates; late in the walking cycle, the big toe may experience high pressures and be pushed out of alignment.
HOW CAN BUNIONS BE TREATED?
Early identification and management will help to reduce the amount of deformity caused. At Footmotion, our highly skilled Podiatrists will thoroughly assess the contributing factors. This will include assessing the extent of the deformity, muscle strength around the joint, the way you walk (may involve a biomechanical examination and computerised gait analysis) and checking your footwear. A comprehensive management programme may include:
- Supportive, well-fitting footwear for work, sport or leisure
- Exercises to stretch and strengthen the muscles around the joint
- Protective padding, including customised silicon devices to wear in shoes
- Braces and splints that are worn at night
- Arch supports or prescription orthoses for foot support and correction of walking patterns
- Coordinating care with other health professionals as required, for example referral for xrays if needed
In our experience, most people can get relief of the pain quickly. Contact us today to book your appointment. At your visit, be sure to bring examples of your work, sports and leisure shoes so the podiatrist can give you the right advice straight away.
1. Nix et al (2010)
2. Nix et al (2012)
 WHAT IS PLANTAR FASCIITIS?
WHAT IS PLANTAR FASCIITIS?
Plantar Fasciitis (or fasciosis) is one of the most common causes of foot pain, with 1 in 10 of us experiencing it at least once in our lifetime. It involves pain at the heel near the origin of the plantar fascia, a tight connective tissue band that runs from the calcaneus (heel bone) to the ball of the foot. Sometimes the pain can be located towards the middle of the arch.
Plantar Fasciitis is a degenerative condition characterised by thickening of the fascia and sometimes heel spurs.
Most people report heel pain first thing in the morning or after periods of rest that improves with a little walking. It can also be brought on if you are standing for long periods or with exercise.
WHAT CAUSES PLANTAR FASCIITIS?
You may develop plantar fasciitis if you have:
- Flat or pronated feet
- High arch feet
- Excessive weight
- Non-supportive footwear
- Prolonged standing/walking occupations
- Tight Achilles tendon and foot muscles
- Excessive running or exercise
- Pregnancy
- Some inflammatory conditions
At FootMotion, we use our extensive clinical experience and state-of the-art technology to properly diagnose your foot pain, carry out a biomechanical assessment to accurately assess your foot function and create an evidence-based treatment plan to effectively manage your condition.
HOW CAN PLANTAR FASCIITIS BE TREATED?
Whilst Plantar Fasciitis can be self-limiting and settle within 12-18 months, the pain can be debilitating, limiting your activity. Treatment is often required to ease your pain and prevent recurrence.
At FootMotion Podiatry we rule out other causes of heel pain then customise a treatment programme for you that would include a combination of the following:
- Icing, massage and rest
- Stretching and strengthening exercises
- Strapping
- Supportive, well-cushioned footwear
- Arch supports or prescription orthoses
2. Landorf, KB, McMillan, AM, Menz, HB 2013, Plantar heel pain: an update of its aetiology and diagnosis, Journal of Foot and Ankle Research, vol. 6 Suppl. 1 p. 18.
3. Fink, BR 2012 Management of Plantar Fasciitis Evolving, The Journal of Musculoskeletal Medicine 29, pp.16-20
4. Nicholl, D 2009, Plantar fasciitis: Part 2: recommendations for best clinical practice for the evaluation and treatment of plantar fasciitis Podiatry Now vol. 12, no. 1, p. 13
 WHAT IS ARTHRITIS?
WHAT IS ARTHRITIS?
Arthritis is a general term used to describe any type of joint pain. It is usually associated with pain, stiffness, inflammation and joint damage.
There are many different types of arthritis, with the most common being Osteoarthritis and Rheumatoid Arthritis. Gout is also a form of arthritis. These three forms of arthritis account for 95% of arthritis cases in Australia. However there are around 100 different types of arthritis and they can affect any age group. Arthritis generally becomes more prevalent with age, particularly after the age of 45 years.[1]
Just about any joint in the body can be affected by arthritis, and with 33 joints in each foot, it isn’t surprising that arthritis in the feet is pretty common. In fact, about 1 in 6 older people had painful arthritis affecting their feet according to a recent study.[2]
Knees, hips and spine are also quite susceptible to developing arthritis. Being overweight places more stress on the bones and joints and has been shown to increase foot and lower limb pain in arthritis.
HOW IS ARTHRITIS TREATED?
Treatment for arthritis depends on the exact type of arthritis and the joints affected.
Generally speaking though, when treating arthritis associated with your feet and legs, treatment usually involves:
- Stretches and exercises to maintain joint mobility
- Supportive, well cushioned footwear, fitted well to protect painful joints
- Arch supports or prescription orthoses to stabilise the foot, reduce abnormal joint loading and help prevent deformity
- Advice for maintaining healthy lifestyle and reducing stress on the affected joints
1. AIHW, A snapshot of arthritis in Australia 2010, 2010, Australian Institute of Health and Welfare Canberra.
2. Roddy, E., et al., The population prevalence of symptomatic radiographic foot osteoarthritis in community-dwelling older adults: cross-sectional findings from the clinical assessment study of the foot. Annals Of The Rheumatic Diseases, 2015. 74(1): p. 156-163.
 WHAT ARE PLANTAR WARTS?
WHAT ARE PLANTAR WARTS?
Plantar Warts (or verrucae) are warts that occur on the bottom of your feet. They generally appear as hard lumps in the skin with thick skin surrounding it. They are often mistaken for corns but can be differentiated by the appearance of small black dots in the middle of the wart and with the lack of skin striations (skin lines on the feet, like fingerprint lines) through the wart.
Plantar Warts can occur at any age but are particularly common in school-aged children. [1] They are contagious and can be spread when using communal facilities such as change rooms and showers.
Plantar Warts are sometimes painful, depending on their location on your foot and how big or how deep they are. The decision to treat them is usually dependent on whether they are painful.
WHAT CAUSES PLANTAR WARTS?
Plantar warts, like any wart, are caused by the Human Papilloma Virus (HPV). There are over 100 different strains of HPV, with only a few causing warts on your feet. The virus enters the body through a small break in the skin surface [2], however, the virus can remain dormant in the body and become evident months, if not years later.
Pain associated with warts is due to the pressure applied to the soft tissue underneath the wart, as the wart and surrounding callus gets thicker.
HOW CAN PLANTAR WARTS BE TREATED?
Often warts will resolve on their own without any treatment, but this may take years to do so. Treatment options for Plantar Warts are quite varied. They range from doing nothing at all, to home remedies such as ‘over the counter’ wart treatments and duct tape, to more advanced treatments such as salicylic acid and cryotherapy (freezing). Surgical removal is also an option. Whatever the treatment, care must be taken to avoid scarring which can sometimes lead to long term painful callus formation.
Research has suggested the best form of treatment for warts is the use of salicylic acid and/or cryotherapy.
Salicylic acid, as the name suggests, is an acid which softens the wart tissue, and with the aid of manual removal of dead skin, will gradually reduce the wart tissue. It is also thought that partially-damaged cells expose the immune system to HPV to stimulate your body’s immune system into reacting to the wart too.[1] Care must be taken only to apply the acid to the wart tissue, hence this is often done by your Podiatrist or doctor who may also mask the surrounding area with tape or dressings to protect the healthy skin.
Cryotherapy utilises liquid nitrogen to freeze the wart tissue, and like salicylic acid, will eventually decrease the wart size as well as stimulating your body’s immune system to respond. It can be painful and also requires care taken to ensure only wart tissue is treated.
Silver nitrate has also been shown to have some good results for treating warts. It is also a topical treatment which is painted on to the wart.
All of these non-surgical wart treatments require several applications, and may take weeks or months to resolve, so patience and persistence is key. As they all cause tissue damage, these treatments must be used with great caution in people who have poor circulation or sensation e.g. diabetes or those who have poor immunity. In some of these cases no treatment may be the best option.
At FootMotion, we use our extensive clinical experience and state-of the-art technology to properly diagnose your skin condition, carry out a thorough vascular and neurological examination to accurately assess your foot health and create an evidence-based treatment plan to effectively manage your condition.
WHAT IS HEEL PAIN?
Your heel bone (calcaneus) is the largest bone in your foot. It takes the bulk of the foot’s forces during heel strike when you are walking, leaving it prone to injury. There are many different conditions which cause of heel pain, including:
- Plantar fasciitis
- Heel spurs
- Achilles tendonitis
- Fractures
- Sever’s disease (in children)
- Plantarfibromatosis
- Nerve entrapments
WHAT CAUSES HEEL PAIN?
As mentioned above, there are several different conditions that can cause your heel pain. Other contributing factors include:
- Flat feet
- High arch feet
- Excessive weight
- Standing or walking for prolonged periods on hard surfaces
- Non-supportive footwear
- Tight Achilles tendon and foot muscles
- Some inflammatory conditions
 At FootMotion, we use our extensive clinical experience and state-of the-art technology to properly diagnose your foot pain, carry out a biomechanical assessment to accurately assess your foot function and create an evidence-based treatment plan to effectively manage your condition.
At FootMotion, we use our extensive clinical experience and state-of the-art technology to properly diagnose your foot pain, carry out a biomechanical assessment to accurately assess your foot function and create an evidence-based treatment plan to effectively manage your condition.
HOW CAN HEEL PAIN BE TREATED?
Treating your pain involves making a clear diagnosis of the cause of your pain and then developing a tailored treatment programme to effectively reduce your pain.
This may include:
- Icing, massage and rest
- Stretching and strengthening exercises
- Strapping
- Supportive, well-cushioned footwear
- Arch supports or prescription orthoses
 Fractured Toes are quite common, and can result from a direct blow to the foot, for example, the accidentally kicking something hard or dropping a heavy object on your toes.
Fractured Toes are quite common, and can result from a direct blow to the foot, for example, the accidentally kicking something hard or dropping a heavy object on your toes.
They can also result from the overuse and repetitive stress that comes with participating in high-impact sports like running and rugby. Toe and forefoot fractures often result from trauma or direct injury to the bone.
Fractures can also develop after repetitive activity, rather than a single injury. This is called a “stress fracture.” Fractures may either be “non-displaced,” where the bone is cracked but the ends of the bone are together, or “displaced,” where the end of the broken bones have partially or completely separated.
Although fracturing a bone in your toe or forefoot can be quite painful, it rarely requires surgery. In most cases, a toe fracture will heal with rest and a change in footwear.
 WHAT IS AN INGROWN TOENAIL?
WHAT IS AN INGROWN TOENAIL?
An ingrown nail is a common condition affecting the toes, most often the big toes. It occurs when the side or corner of the nail digs into the skin alongside your nail and causes pain and irritation with the potential for the skin to become inflamed and infected. An involuted (excessively curved) nail can cause similar problems with pain, inflammation and infection. The curved nail presses on the tissues of the nail bed or the sulci (grooves) along the edges of the nail plate or both.
WHAT CAUSES AN INGROWN NAIL?
The main causes of ingrown toenails include:
- Incorrect cutting of nails, such as cutting them too short, not cutting straight across to remove the sharp corner, or tearing or picking them
- Injuring your toe
- Wearing shoes that are too tight or short
- Having nails that naturally curve more than usual
- Pressure between the toes due to bunions or toe deformities
Left untreated, an ingrown toenail can become infected which may lead to deeper infection in the tissue and bones if it is neglected or in people who have certain medical conditions such as diabetes. Even if an ingrown toenail becomes infected and you are given antibiotics by your doctor, it is important to have the problematic section of nail is removed to allow the toe to heal and prevent its recurrence.
At FootMotion, we use our extensive clinical experience and state-of the-art technology to properly diagnose your skin and nail condition, carry out a thorough vascular and neurological examination to accurately assess their foot health and create an evidence-based treatment plan to effectively manage your condition.
HOW CAN AN INGROWN TOENAIL BE TREATED?
In many cases, the troublesome toenail can be conservatively managed by removing just the small section of the nail that is causing the problem. Antiseptics and in some cases antibiotics may be needed in the case of an infection. Our Podiatrists have techniques to minimise your discomfort while treating your ingrown toenail. In some cases, we can administer a local anaesthetic to temporarily numb the area being treated.
Surgical Intervention
When there are recurring ingrown toenails or if the ingrown toenail is severe, we may suggest surgery to permanently remove part of the nail that is causing the problems. This procedure, called a nail wedge resection, involves removing a small section along the edge of the nail, narrowing the nail width slightly. The nail root or ‘matrix’ is then cauterised with a chemical to prevent the regrowth of the nail. It is a relatively simple procedure, performed by our Podiatrists in our clinic rooms with strict infection control procedures followed. According to a large clinical study, this particular technique is very effective at correcting the problem permanently. [1] It does require a local anaesthetic, however you will be able to walk out of the clinic room and generally won’t require an extended time recovery time. Nail Bracing – a non-surgical intervention
Nail Bracing – a non-surgical intervention
Where a non-surgical correction is medically advisable or a personal preference, Footmotion Podiatry offers nail bracing as an effective alternative for nail surgery. Nail bracing can alleviate discomfort quickly and painlessly. As no local anaesthetic is used nail bracing is suitable for children and people with diabetes. Where the treatment aim is to re-shape a curved nail plate the bracing may be removed and reapplied at regular intervals over a period between 3 to 12 months.
GENERAL ADVICE AND HOME CARE
To help avoid the ingrown toenails in future, you will be shown ways to reduce the risk of them returning. This may include:
- Advice on how to cut and care for your nails
- Footwear review and advice to ensure proper fit and support
- Ongoing nail care by our Podiatrists to help with difficult nail shapes
- Treatment for foot conditions such as bunions and toe deformities

Our Services
Did you know your feet will travel 128,000 kms or more in a lifetime, equivalent to walking three times around the world? [1] It’s little wonder that according to one Australian study just under 20% of us report having foot aches, pain or stiffness most days.[2]
People who reported knee, hip and back pain were also more likely to also have foot pain. At Foot Motion, people come to see us for help with a wide range of concerns about their feet and legs. We offer podiatry services and advice on foot health issues such as:
- Foot pain, aches, stiffness
- Foot conditions such as heel pain, bunions, metatarsalgia, flat feet and high arched feet
- Foot and lower limb problems caused by medical conditions such as arthritis, gout and diabetes
- Skin and nail conditions such as fungal nails, ingrowing nails, corns, callous and tinea
- Difficulty with footwear
- Foot problems at work
 OUR GENERAL PODIATRY SERVICES
OUR GENERAL PODIATRY SERVICES
If you don’t have pain but you do have concerns regarding your foot and leg alignment or function, our Podiatrists can certainly take a look and provide you with feedback and advice about how to improve your lower limb function. It may be that you have a family history of foot and leg problems and want advice on how to avoid these yourself – we can help! We conduct a thorough Biomechanical Examination and Gait Analysis to provide you with a detailed overview of the way your feet and legs work and advice on how to prevent problems developing in the future.
If shoes are a problem, we can provide you with advice and help you select appropriate shoes for your feet. We are also happy to provide you with General Podiatry services including care for hard to manage nails and skin problems (such as callus and corns) and have effective treatments for ingrown toenails and warts.
At FootMotion, we see patients across all age groups, from little kids to our seniors, and with all levels of activity. No problem is too big or too small. If you have concerns about your feet or legs, having a check up from a FootMotion podiatrist is the place to start.
2. Hill, C.L., et al., Prevalence and correlates of foot pain in a population-based study: the North West Adelaide health study. Journal Of Foot And Ankle Research, 2008. 1(1): p. 2-2.
STATE OF THE ART EQUIPMENT To enhance management of your foot health, we have sourced state-of-the-art systems for measuring function and posture of your feet and for detailed analysis of your gait and balance.
To enhance management of your foot health, we have sourced state-of-the-art systems for measuring function and posture of your feet and for detailed analysis of your gait and balance.
The Zebris computerised gait and stance analysis system incorporates pressure plate sensors inbuilt into a treadmill with synchronised video streaming to provide the ultimate analysis of your walking and running gait as well as balance assessment.
We also use the TOG GaitScan system which is perfect for anybody who is not confident walking on a treadmill. These systems provide our podiatrists with a wealth of detailed and accurate information about your foot and lower limb function, so they can give you the best advice possible.
IN THE HANDS OF CARING, EXPERIENCED PROFESSIONALS
In addition to using the latest gait analysis technologies, our podiatrists can perform a detailed biomechanical examination of your feet and lower limbs, as well as your standing posture.
With this examination we measure of the movement and alignment of your joints, your muscle strength and overall foot function to provide a complete overview of your total foot and leg function and alignment.  WHAT TO BRING FOR YOUR BIOMECHANICAL EXAMINATION
WHAT TO BRING FOR YOUR BIOMECHANICAL EXAMINATION
If you have an appointment for a Biomechanical Examination and Gait Analysis, it is handy to bring with you a pair of shorts (or pants that can be rolled up comfortably to your knees) and the shoes that you wear most often for work and exercise.
If you have diabetes or another condition affecting your foot sensation or circulation, you will benefit from our comprehensive diabetes foot protection programme. The programme uses the foot assessments recommended expert guidelines and adds additional assessments based on up to date research and the latest technology. At Footmotion, your programme includes:
- Neurological assessment
- Vascular (circulation) assessment
- Assessment of foot shape and deformity using physical examination and 3D laser scanning
- Computerised plantar pressure assessment
- Footwear assessment and advice
- Foot care education
ABOUT OUR DIABETES FOOT PROTECTION PROGRAMME Neurological Assessment
Neurological Assessment
People with intermediate or high risk feet in diabetes usually have decreased sensation due to peripheral neuropathy (nerve damage). Peripheral neuropathy can be of two main types- sensory and motor [2]. Sensory neuropathy affects the sensory nerves (those responsible for feeling) and can produce numbness, tingling or even increased sensitivity and pain in your feet. Motor neuropathy affects the nerves that control the muscles and can lead to muscle weakness, which in turn can produce deformity of your toes and feet. The neurological assessment includes a range of clinical tests.
At Footmotion, we use one of the most widely recommended tests for neuropathy – the monofilament test. If you can’t feel the monofilament you will not be able to detect a foot injury in that area of your foot and will need to take special precautions to protect that area.
Vascular (Circulation) Assessment
Diabetes can also cause peripheral arterial disease (PAD), previously referred to as peripheral vascular disease (PVD) [2] . Peripheral arterial disease can result in reduced blood flow to your feet and legs which can cause pain in the feet or legs with walking or even when at rest. People without diabetes can also develop PAD, particularly when there is a history of smoking.
At FootMotion as part of our Diabetes Foot Protection Program the podiatrist will check your circulation beginning with feeling the pulses in the feet and ankles. Often the Doppler ultrasound is used to measure the blood pressure at the ankle and the arm. The guidelines recommend an ankle-brachial index or ABI to be calculated. The ideal ABI is 1.0, which means there’s no drop in blood pressure at the ankle compared to the arm and hence minimal/no damage to the large arteries in the leg/ankle. If the podiatrist requires more information about your blood flow below the ankle they may use another test called photoplethysmography or PPG. This test can detect the blood flow through the smaller arteries to the skin, by placing a sensor on your toes. A Toe-Brachial Index can be determined-TBI, similar to the ABI. Another acceptable PPG test we use is an Absolute Toe Pressure (ATP).
If the podiatrist requires more information about your blood flow below the ankle they may use another test called photoplethysmography or PPG. This test can detect the blood flow through the smaller arteries to the skin, by placing a sensor on your toes. A Toe-Brachial Index can be determined-TBI, similar to the ABI. Another acceptable PPG test we use is an Absolute Toe Pressure (ATP).
Assessment Of Foot Shape And Deformity
Diabetes can cause a number of changes in foot shape, structure and movement including collapse of the arch, development of toe deformities and stiffening of the joints in the foot due to changes in the ligaments. Wasting of the soft tissues and padding beneath the foot can make the metatarsal heads and heel bones more prominent and susceptible to injury. Muscle weakness can also change the shape of the foot. FootMotion podiatrists conduct a visual and physical examination of your foot to identify the onset of these problems. At Footmotion, we have a state-of-the-art 3D laser scanner which is able to measure the shape and dimensions of your feet with the highest levels of accuracy. This is allows FootMotion podiatrists to identify subtle differences between your feet and to monitor your foot structure over time – providing early warning of changes. Patients receive a copy of the scanner results.
At Footmotion, we have a state-of-the-art 3D laser scanner which is able to measure the shape and dimensions of your feet with the highest levels of accuracy. This is allows FootMotion podiatrists to identify subtle differences between your feet and to monitor your foot structure over time – providing early warning of changes. Patients receive a copy of the scanner results.
Computerised Plantar (Sole) Pressure Assessment
Foot deformities and changes in the soft tissues of the feet can lead to high pressure areas under the sole of your foot during walking. Often this can lead to callous formation and once callouses develop, they can increase the stress under the foot even further [4] which can lead to ulceration. FootMotion podiatrists perform a computerised plantar pressure assessment to measure high pressure areas under your foot as you take a step. Once these areas are identified, the podiatrists can prescribe changes to footwear and shoe insoles or foot orthoses to reduce these pressures.
FootMotion podiatrists perform a computerised plantar pressure assessment to measure high pressure areas under your foot as you take a step. Once these areas are identified, the podiatrists can prescribe changes to footwear and shoe insoles or foot orthoses to reduce these pressures.
It is essential that everyone at risk of foot ulcers has their feet and shoes checked for signs of high plantar pressures.
Footwear Assessment And Advice
Foot deformities such as bunions and hammer toes can affect shoe fitting and many people wear shoes that are the wrong size for their feet. Foot deformity and footwear are key contributors to ulceration risk and 35-50% of foot ulcers may have been caused by inappropriate footwear according to some studies [3]. Shoes with extra depth, good cushioning and support are important for protecting feet in diabetes. It is essential that everyone at risk of foot ulcers has correctly fitting footwear. Once the podiatrists have conducted the assessments of your foot shape and looked at the plantar pressures they will provide individualised footwear recommendations for you as part of the diabetes foot protection program.
Some of the latest research suggests it is important to keep the plantar pressures below 200 kPa to prevent foot ulcers [5]. We know that shoes with a rocker sole, custom moulded insoles, metatarsal pads or arch support orthoses can help to reduce plantar pressures [6]. One study found that custom shoes with different combinations of metatarsal pads, localised cushioning under problem areas of the foot and extra cushioned insoles could further reduce plantar pressures by as much as 24% [5]. So we can see that there are many ways that the podiatrist can reduce the pressures under your feet and bring them to a safe level.
Foot Care Education
Once your foot assessments and footwear evaluation are completed, the podiatrist, as part of our Diabetes Foot Protection program will talk with you about the most important findings. They will discuss with you how diabetes can affect the feet, highlight any current problems and discuss appropriate treatment options. They will also talk with you about a home foot care routine you can use to keep your feet healthy.
If you have diabetes or you are concerned about the circulation or sensation in your feet the Comprehensive Diabetes Foot Protection Program is designed for you. Our expert staff will use the latest technology and evidence-based techniques to assess your feet and give you the best advice we can on preventing foot problems in the future.
Call the Clinic and start protecting your feet TODAY with our Diabetes Foot Protection Program.
2. Australian Institute of Health and Welfare, Diabetes Australian Facts, 2008, Australian Government: Canberra.
3. National Health & Medical Research Council, National Evidence-Based Guideline on Prevention, Identification and Management of Foot Complications in Diabetes (Part of the Guidelines on Management of Type 2 Diabetes), 2011, Baker IDI Heart & Diabetes Institute: Melbourne.
4. Hamatani, M., et al., Factors Associated With Callus in Diabetic Patients, Focused on Plantar Shear Stress During Gait. Journal Of Diabetes Science And Technology, 2016.
5. Arts, M.L.J., et al., Data-driven directions for effective footwear provision for the high-risk diabetic foot. Diabetic Medicine: A Journal Of The British Diabetic Association, 2015. 32(6): p. 790-797.
6. Bus, S.A., et al., Footwear and offloading interventions to prevent and heal foot ulcers and reduce plantar pressure in patients with diabetes: a systematic review. Diabetes/Metabolism Research And Reviews, 2016. 32 Suppl 1: p. 99-118.
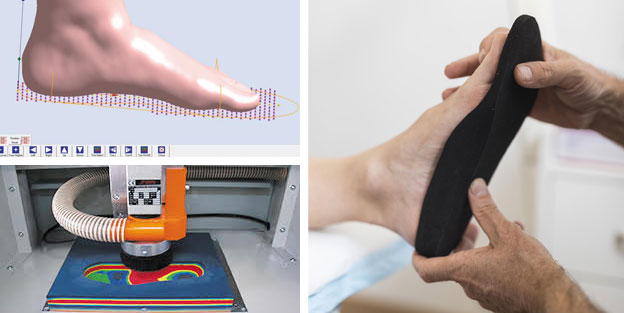
After a comprehensive biomechanical assessment and gait analysis, foot orthoses may be indicated as part of your care programme.
Our 3D CADCAM technology ensures a quick turnaround time for accurate, comfortable and functional orthotics, made from the highest quality medical grade materials.
THE BENEFITS OF CUSTOM ORTHOSES
The benefits of wearing custom orthotics include:
- Maintains correct foot and leg alignment
- Improves balance
- Offers greater supports to the arch and heel
- Can prevent bunions and clawed digits
- Absorbs shock and redistributes pressure and weight across the entire foot
- Can prevents subsidiary foot conditions like corns, calluses and ulcerations by offloading pressure from risk areas
- Reduces fatigue
- Can alleviate pain in the feet, ankles, legs, and lower back
 INGROWN TOENAIL TREATMENT
INGROWN TOENAIL TREATMENT
Ingrown toenails can be very painful. That’s why our FootMotion Podiatrists have developed techniques to minimise your discomfort while treating your ingrown toenail.
In many cases, the troublesome toenail can be conservatively managed by removing just the small section of the nail that is causing the problem. Where the problem is due to an involuted (excessively curved) nail, treatment may include nail packing to separate and elevate the nail from the surrounding tissues, thus reducing pressure and pain. You will be shown ways to help reduce the risk of the ingrown toenail returning.
In cases where there are recurrent ingrown toenails or if the ingrown toenail condition or nail shape is severe, we may suggest either surgical intervention or the application of a nail brace.
SURGICAL INTERVENTION
The aim of surgical treatment for an ingrown toenail is to permanently remove part of the nail that is causing the problems. This procedure, called a nail wedge resection, involves removing a small section along the edge of the nail, narrowing the nail width slightly. The nail root or ‘matrix’ is then cauterised with a chemical to prevent the regrowth of the nail. It is a relatively simple procedure, performed by our Podiatrists in our clinic rooms with strict infection control procedures followed. According to a large clinical study, this particular technique is very effective at correcting the problem permanently. [1] It does require a local anaesthetic, however you will be able to walk out of the clinic room and generally won’t require an extended recovery time.
Where a non-surgical option is best or preferred, Footmotion Podiatry offers nail bracing that requires no anaesthetic and no recovery time.
NAIL BRACING – A NON-SURGICAL INTERVENTION
Nail bracing can alleviate discomfort from ingrown or involuted nails quickly and painlessly. Nail bracing aims to correct the shape of the deformed nail plate, reducing the pain from the pressure on the nail bed. Small medical grade wires are fastened across the nail surface and glued in place. The nail brace acts to elevate the nail plate and unload the pressure on the underlying skin and along the nail groove while reforming the nail plate placed under tension.
As no local anaesthetic is used nail bracing is suitable for children and people with diabetes. Where the treatment aim is to re-shape a curved nail plate the bracing may be removed and reapplied at regular intervals over a period between 3 to 12 months.
Our Podiatrists can discuss these treatment options with you in more detail.
Many foot and lower limb problems are helped and even resolved with appropriate functional footwear. Our podiatrists will provide you with personalised recommendations after thoroughly assessing your needs.
In our co-located retail store, our fitting professionals utilise world-leading 3D technology to ensure your foot is matched to the right shoe.
ABOUT OUR FOOTWEAR
Our extensive range includes running shoes, work shoes, sandals and casual footwear. All are suitable for wearing with orthotics and we go to great lengths to offer all sizes at all times to ensure that you will receive the best possible fit.
Our stocked range includes selected seasonal styles from brands such as; NIKE, Muzuno, ECCO, Ascent, Vionic, Revere, HOKA One One, KEEN, Salomon, Dansko, Aetrax, Teva, OluKai and Ahnu. This extensive range ensures not only the best available fit but also offers a stylish and functional shoe for your every need.

TAILORED EXERCISE PROGRAMS
Improving foot health and function doesn‘t stop with new shoes and possibly arch supports. Exercise is an integral part of ensuring good muscle strength and flexibility in both your legs and feet and is crucial to your overall comfort and recovery.
At FootMotion, our Podiatrists will coach you through foot and leg stretches as well as providing you with basic strengthening exercises as part of your total management. We also have a network of other health and fitness professionals who we can refer you to when a more tailored program is required.
An exercise program that is tailored specifically to your needs is a great way to stay physically fit. It also provides additional benefits such as:
- Increased muscular strength, endurance and motor fitness
- Increased aerobic fitness
- Improved muscle tone and strength
- Better coordination, agility and flexibility
- Improved balance and spatial awareness

 A Chronic Disease Management Plan is an Australian Commonwealth Government initiative where people with a chronic medical condition may be able to receive Medicare benefits towards the costs of podiatry care to help manage their condition. This scheme was formerly known as the Enhanced Primary Care (EPC) Programme. This requires a referral from your GP who will determine if you are eligible for the programme.
A Chronic Disease Management Plan is an Australian Commonwealth Government initiative where people with a chronic medical condition may be able to receive Medicare benefits towards the costs of podiatry care to help manage their condition. This scheme was formerly known as the Enhanced Primary Care (EPC) Programme. This requires a referral from your GP who will determine if you are eligible for the programme.
At FootMotion, we accept management plan referrals and provide your GP with the relevant reports of your progress.
CHRONIC DISEASE MANAGEMENT PLAN
Talk to your doctor to find out more about the plan and your eligibility. Some conditions covered by the initiative that FootMotion can aid with include diabetes, musculoskeletal conditions and stroke rehabilitation.
You can read more about chronic disease management plans at the Australian Government Department of Health website, simply visit: www.health.gov.au
ABOUT OUR BALANCE ASSESSMENT
Postural balance is the ability to keep the body centre of mass within the base of support, so that the rapid displacement of the body mass may occur coordinately in different directions. This requires constant adjustments of muscular activity and articular positioning Using our state-of-the-art balance assessment analysis systems, we are able to evaluate your overall balance both in natural stance and in gait.
Our computerised analysis equipment can show you where the centre of pressure is under your body, how much your body sways and how fast it sways when your balance is challenged. Your data and postural control is evaluated. Assessing this information and your postural control can be used to recommend strategies to improve your body balance and measure your progress along the way.
Improving your body balance can be helpful in falls prevention and highlights theimportance of balance assessment.

FAQs
If you are eligible for the Chronic Disease Management Program (formerly known as the Enhanced Primary Care (EPC) Scheme) you will be able to pay the full consultation fee and receive a partial benefit from Medicare. Please discuss this program with your GP who will determine if you are eligible.
No, for the majority of podiatry related problems you do not require a doctor’s referral. Simply make an appointment to see one of our Podiatrists. A current doctor’s referral will be required if you are eligible to have your treatment covered by WorkCover, The Department of Veterans’ Affairs (DVA), or The Chronic Disease ManagementScheme through Medicare (formerly known as Enhanced Primary Care (EPC) Scheme).
Podiatry services are usually covered by Private Health Insurance Extras but you will need to check the details of your individual policy with your health fund. Throughout your treatment, we can provide you with individual item numbers to help you check with your fund. We have on-the-spot health fund claiming available at the practice.
Our street address is 3 Sherwood Road, Toowong. FootMotion is conveniently located in front of the Toowong Station, next to Toowong Village. You can walk up the stairs from Nando's to find us! Podiatry is on the right hand side next to our retail store.
There is parking located downstairs in the car park below us for clients, or you can park inside Toowong Village and walk over.
At your first appointment, it’s helpful to bring a selection of your current footwear, particularly any that you are having problems with. Orthotics, if you have any. Any x-rays or scans you may have of your feet or legs. Comfortable clothing, as we may have you walking and moving around to examine your feet and legs.
Fees vary depending on the type of treatment required. Please call our clinic and we will be happy to discuss what costs may be involved depending on your particular needs.
The length of your appointment depends on the type of treatment you require. A first appointment usually takes 40 minutes. Arriving 10 minutes before this first appointment will also allow time to get your paperwork done so we can take you through promptly.